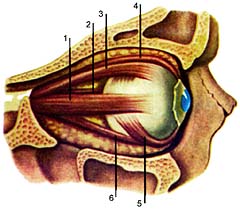
An investigation of oculomotor muscles
All oculomotor function are studied in the middle position of the head and look at the patient directly (primary position).
Attention is drawn to the width of the eye slits of their value. Normally, the upper lid should not go to the area of the pupil. If it comes, it is ptosis (or poluptoz).
To investigate the function of muscles, elevating the upper eyelid (for Burke), pressing the finger skin in eyebrows, asked to look up. If you look up eye gap widened, then the function levatora partially preserved. Further attempts to unscrew the upper eyelid. If it is not twisted, it may indicate a complete paralysis levatora.
Exophthalmometer performed by a special device (exophthalmometer), which is determined vystoyanie eyeballs (exophthalmos, endophthalmitis).
Determines the angle of strabismus on the implementation Hirschberg covegtest (cvt). A light beam is directed to mirror the patient's eyes light reflex should be symmetrical on the right and the left pupil, pass almost through the center of the pupil.
If the reflex in one eye asymmetric another, then we are dealing with strabismus (geterotropiey). The magnitude of deviation is determined by the scheme:
"+" sign indicates esotropia (intropiya);
sign "" denotes exotropia (ekzotropiya);
"1 or 1" vertical strabismus.
Covering it right, then left eye, then removing the palm (covegtest), we determine deviation of the right and left eyes.
The recording is done as follows:
Dev. +10 (Angle right and left eyes are equal) ODOS;
Dev. 1S20 (the angles are not equal).
Oftalmodinamika investigated the scheme Ebert.
We investigate the direct and friendly response of pupils to light: a doctor with his hand that covers the patient's eye (the pupil of the eye covered with expanded), then opens it (the pupil opens his eyes narrowed) a direct reaction to light. It draws attention to the behavior of another pupil. The reaction of the pupil of the second eye coincides with the reaction of the opened eyes (friendly reaction). No
friendly response to light indicates a failure of parasympathetic fibers in the longitudinal beam.
Checks the reaction of the pupil to convergence. This patient is invited to look at the neurological hammer, shifted to 50-60 cm hammer slowly coming to the nose of the patient. B is the norm convergence of the axes of the eyeballs (convergence) with simultaneous narrowing of the pupils. Most pupillary constriction is observed at a distance of 1 – 15 cm Lack of response to the convergence of interpretation of the defeat of the longitudinal beam.
Investigate the reaction of pupils to accommodations (checked in one eye, the other closed). Normally, the pupillary constriction is noted when considering the subject near and extension when viewed from afar.
Investigate the reaction of pupils to pain. When pain stimulation of any part of the body marked mydriasis on the side of pain (a symptom Parry). Lack of expansion of the pupil on the pain indicates injury of the sympathetic innervation of the pupil.
Symptoms defeat
Central paralysis of eye muscles occur in defeat kortikonuklearnyh tract are rare because of bilateral innervation of the nuclei of oculomotor nerves. In the central paralysis (paresis) is a gaze paresis, ie narrowing. restriction of the binocular field of gaze.
Central paralysis have 2 features:
1) affects both eyes;
2) 2 or 4 muscles (synergists) are in a state of spasm, and their antagonists in a state of extreme relaxation (atonic).
Eyes are always «turned to the lesion focus. If suffering and pyramidal path, then turned his eyes on the hearth, but «of hemiplegia. Options include violations acsotsiirovannyh eye movements:
supranuclear gaze palsy to the right:
1) eyes turned to the left;
2) the forced rotation of the head (tortikollis) to the left;
3) horizontal motion is not available;
4) vertical motion in full;
supranuclear gaze palsy to the left:
1) eyes turned to the right;
2) forced head turn to the right;
3) horizontal motion is not available;
4) vertical motion in full;
nadyaderny paralysis gaze up:
1) eyes lowered down;
2) head lowered;
3) horizontal motion in full;
4) vertical motion are absent.
Flaccid paralysis of eye muscles, regardless of cause, they have been called, lead to the development of strabismus. Strabismus in turn is polietiologicheskim disease caused by not only the paralysis of eye muscles. Therefore, when formulating a diagnosis would be correct to write: a convergent (divergent, vertical), crossed eyes, paralysis of certain muscles (but not paralytic strabismus, as was the earlier).
The angle of strabismus before they develop some atrophy, hypertrophy of other muscles, usually not expressed. The only complaint in the early stages of a diplopia (double vision), which is explained by the fact that the squint light rays excite asymmetric, disparate, areas of retinas double vision can lead to poor general condition in dizziness, nausea and vomiting. Patient copes with
diplopia, screwing up one eye, rejecting his head in the direction where the doubling less. Usually diplopia there a short time, the body itself helps to cope with it suppressed images of (mostly mowing) eyes at the level of the cerebral cortex.
TRANSLATE FROM RUSSIAN BY GOOGLE